Hemifacial spasm (HFS) is an involuntary twitching in the area of one side of the face.
The disease itself has no health consequences. However, it places a heavy psychological strain on patients, as those affected often withdraw from public life.
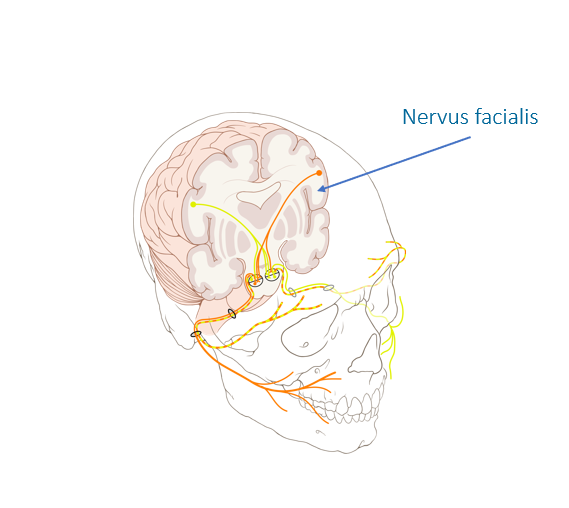
The cause of this disease is a vessel-nerve contact that damages the “isolation” (Schwann cells) of the facial nerve (nervus facialis). However, hemifacial spasm must be distinguished from other conditions such as synkinesia (involuntary movement disorders) following paralysis of the facial nerve, facial tic, blepharospasm, oromandibular dystonia, and other facial spasms before specific treatment can be planned.
Patients with hemifacial spasm experience involuntary and unwanted facial twitching in one side of the face, usually beginning very discretely and increaseing significantly as the condition progresses.
In case of a hemifacial spasm, a detailed anamnesis (medical history) and extensive interdisciplinary diagnostics by neurosurgeons, neurologists and ENT physicians must always be performed.
In addition, neuroradiological imaging in the MRI (“tube”) must be performed. Thin-slice MRI images (with a layer thickness of 1 mm or less with contrast media, native and T2 as well as CISS special sequences) are required to visualize the brain nerves and detect vascular nerve contact. Unfortunately, vascular nerve contacts are often not mentioned in the written report. A thin-slice CT of the skull base and the petrous bone (a section of the temporal bone) is usually performed to assess the bony structure.
As conservative therapy, there is only the possibility of a local injection of botulinum toxin. However, this does not remove the cause of the disease, but only the symptoms. The medication is injected into the affected muscle and must be repeated regularly, otherwise it loses its effect.
In most patients suffering from hemifacial spasm, it is not known that the cause of the disease can be permanently eliminated by minimally invasive surgery. Prof. Feigl performs these operations with the support of navigation and endoscopy, and with constant monitoring of the brain nerve currents (intraoperative monitoring).
If necessary, fluorescence angiography can be used during the operation. This uses a contrast medium to make the vessels visible. The goal of the surgery is to place padding under the vascular loop that is attached to the facial nerve. This results in immediate and permanent relief of symptoms in almost all patients.
Hemifacial spasm (HFS) is an involuntary twitching in the area of one side of the face. The disease itself has no health consequences. However, it places a heavy psychological strain on patients, as those affected often withdraw from public life.
The cause of this disease is a vessel-nerve contact that damages the “isolation” (Schwann cells) of the facial nerve (nervus facialis). However, hemifacial spasm must be distinguished from other conditions such as synkinesia (involuntary movement disorders) following paralysis of the facial nerve, facial tic, blepharospasm, oromandibular dystonia, and other facial spasms before specific treatment can be planned.
Patients with hemifacial spasm experience involuntary and unwanted facial twitching in one side of the face, usually beginning very discretely and increaseing significantly as the condition progresses.
In case of a hemifacial spasm, a detailed anamnesis (medical history) and extensive interdisciplinary diagnostics by neurosurgeons, neurologists and ENT physicians must always be performed.
In addition, neuroradiological imaging in the MRI (“tube”) must be performed. Thin-slice MRI images (with a layer thickness of 1 mm or less with contrast media, native and T2 as well as CISS special sequences) are required to visualize the brain nerves and detect vascular nerve contact. Unfortunately, vascular nerve contacts are often not mentioned in the written report. A thin-slice CT of the skull base and the petrous bone (a section of the temporal bone) is usually performed to assess the bony structure.
As conservative therapy, there is only the possibility of a local injection of botulinum toxin. However, this does not remove the cause of the disease, but only the symptoms. The medication is injected into the affected muscle and must be repeated regularly, otherwise it loses its effect.
In most patients suffering from hemifacial spasm, it is not known that the cause of the disease can be permanently eliminated by minimally invasive surgery. Prof. Feigl performs these operations with the support of navigation and endoscopy, and with constant monitoring of the brain nerve currents (intraoperative monitoring).
If necessary, fluorescence angiography can be used during the operation. This uses a contrast medium to make the vessels visible. The goal of the surgery is to place padding under the vascular loop that is attached to the facial nerve. This results in immediate and permanent relief of symptoms in almost all patients.
Understanding Hemifacial Spasm
Understanding Hemifacial Spasm
Request for Treatment
Request for Treatment