Typical anatomical location of an acoustic neuroma
Typical anatomical location of an acoustic neuroma
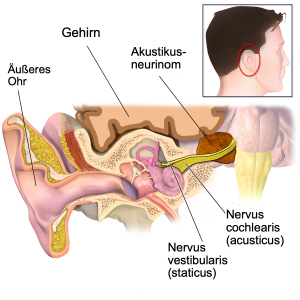
Acoustic neuroma (also: vestibular schwannoma), a benign and usually slow-growing tumor arising from the balance nerve (Nervus vestibularis), usually within the bony auditory canal (Meatus acusticus internus), is one of the most common diseases in the cerebellopontine angle.
Due to the slow increase in size and the suppressive growth, clinical symptoms often appear very late. Because of the tumor’s place of origin, the vestibulocochlear nerve is affected first. Hearing loss, one-sided hearing deterioration, tinnitus and progressive dizziness are common symptoms.
Already with these symptoms, further diagnosis should be performed with electrophysiological examinations (AEP and BERA) and an MRI scan of the skull. Acoustic Evoked Potential (AEP) testing is used to determine the function of hearing using acoustic signals. Brainstem Electric Response Audiometry (BERA) further tests hearing by measuring electrical brain waves. As the tumor grows, the adjacent brain nerves of the cerebellopontine angle also become oppressed, resulting in hypaesthesia (numbness) in the facial area, facial nerve palsy (facial paralysis), and swallowing disorders.
However, large tumors can reach the brainstem or even compress it. This in turn can lead to a rapid deterioration with widespread neurological symptoms and a life-threatening situation. This is because compression of the brainstem leads to blocking hydrocephalus with increasing fluid build-up (fluid circulating in the central nervous system).
A detailed, interdisciplinary diagnosis is required to determine the best individual treatment strategy. This includes a detailed anamnesis (medical history) and a thorough neurological examination as well as an apparative diagnosis. This includes, in particular, the apparative ENT examination: audiogram, speech comprehension and electrophysiological examinations enable an assessment of the vestibulocochlear nerve (eighth cranial nerve, consisting of the balance nerve and auditory nerve) regarding functional impairment.
Detailed neuroradiological imaging by MRI (‘tube’) is always required for acoustic neuroma. Thin-slice MRI images (with a layer thickness of 1 mm or less with contrast media, native and T2 as well as CISS special sequences) are required to identify the cranial nerves with different highlighting. In addition, thin-slice CT of the skull base and petrous bone (a segment of the temporal bone) is performed to assess the bony structure.
‘Wait and scan’ follow-ups
Depending on the patient’s symptoms, regular clinical follow-up with ENT examinations and periodic MRI checks may be recommended when small tumors are first diagnosed. Elderly patients at increased risk of surgery may be encouraged to wait to be screened if there is neither a strong impairment nor evidence of rapid tumour growth. However, for large tumours that carry a the risk of brainstem compression (when the tumour is already pressing on the brainstem), neurosurgical therapy should be performed.
Minimally invasive tumor removal
In the area of the cerebellopontine angle, i. e. between the brainstem, cerebellum and petrous bone, very close anatomical conditions prevail. In addition, there is a very close proximity to the most sensitive neuronal structures. The central parts of ten of the twelve cranial nerves are located here.
The removal of tumours in this region represents a neurosurgical challenge and requires specialization as well as many years of surgical experience and expertise in the field of the skull base, which Prof. Feigl possesses. By using state-of-the-art instruments, Prof. Feigl is able to perform procedures at the base of the skull in a minimal invasive manner via very small and gentle accesses (skull openings).
Stereotactic radiation
Due to the benign and slow growth of acoustic neuromas, conventional radiation is not effective. In this case, high-dose precision irradiation such as Gamma Knife or CyberKnife irradiation (radiosurgery), is required. The goal of this high-precision radiation is to stop the growth of the tumor. Often, the tumour can even be reduced in size a little with this method. However, as with conventional radiation, the surrounding neuronal structures (affecting the nerve cells) must be outside the irradiation field, which is ensured by planning to the nearest millimeter.
Nevertheless, effective radiation of the tumour margins is difficult. Especially in large tumours and in direct vicinity of the brain stem, such irradiation is not possible. In cases of recurrence, repeated radiation therapy is usually possible only to a limited extent. Surgical therapy is extremely difficult in tumors that have already been irradiated because of scarring of the tissue. Prof. Feigl performs radiosurgical treatment of his patients at the Cyberknife Center Southwest in Göppingen. For more information, please visit https://www.radiochirurgicum.de/cyberknife-expertenteam.php.
Acoustic neuroma (also: vestibular schwannoma), a benign and usually slow-growing tumor arising from the balance nerve (nervus vestibularis), usually within the bony auditory canal (meatus acusticus internus), is one of the most common diseases in the cerebellopontine angle.
Due to the slow increase in size and the suppressive growth, clinical symptoms often appear very late. Because of the tumor’s place of origin, the vestibulocochlear nerve is affected first. Hearing loss, one-sided hearing deterioration, tinnitus and progressive dizziness are common symptoms.
Already with these symptoms, further diagnosis should be performed with electrophysiological examinations (AEP and BERA) and an MRI scan of the skull. Acoustic Evoked Potential (AEP) testing is used to determine the function of hearing using acoustic signals. Brainstem Electric Response Audiometry (BERA) further tests hearing by measuring electrical brain waves. As the tumor grows, the adjacent brain nerves of the cerebellopontine angle also become oppressed, resulting in hypaesthesia (numbness) in the facial area, facial nerve palsy (facial paralysis), and swallowing disorders.
However, large tumors can reach the brainstem or even compress it. This in turn can lead to a rapid deterioration with widespread neurological symptoms and a life-threatening situation. This is because compression of the brainstem leads to blocking hydrocephalus with increasing fluid build-up (fluid circulating in the central nervous system).
A detailed, interdisciplinary diagnosis is required to determine the best individual treatment strategy. This includes a detailed anamnesis (medical history) and a thorough neurological examination as well as an apparative diagnosis. This includes, in particular, the apparative ENT examination: audiogram, speech comprehension and electrophysiological examinations enable an assessment of the vestibulocochlear nerve (eighth cranial nerve, consisting of the balance nerve and auditory nerve) regarding functional impairment.
Detailed neuroradiological imaging by MRI (‘tube’) is always required for acoustic neuroma. Thin-slice MRI images (with a layer thickness of 1 mm or less with contrast media, native and T2 as well as CISS special sequences) are required to identify the cranial nerves with different highlighting. In addition, thin-slice CT of the skull base and petrous bone (a segment of the temporal bone) is performed to assess the bony structure.
‘Wait and scan’ follow-ups
Depending on the patient’s symptoms, regular clinical follow-up with ENT examinations and periodic MRI checks may be recommended when small tumors are first diagnosed. Elderly patients at increased risk of surgery may be encouraged to wait to be screened if there is neither a strong impairment nor evidence of rapid tumour growth. However, for large tumours that carry a the risk of brainstem compression (when the tumour is already pressing on the brainstem), neurosurgical therapy should be performed.
Minimally invasive tumor removal
In the area of the cerebellopontine angle, i. e. between the brainstem, cerebellum and petrous bone, very close anatomical conditions prevail. In addition, there is a very close proximity to the most sensitive neuronal structures. The central parts of ten of the twelve cranial nerves are located here.
The removal of tumours in this region represents a neurosurgical challenge and requires specialization as well as many years of surgical experience and expertise in the field of the skull base, which Prof. Feigl possesses. By using state-of-the-art instruments, Prof. Feigl is able to perform procedures at the base of the skull in a minimal invasive manner via very small and gentle accesses (skull openings).
Stereotactic radiation
Due to the benign and slow growth of acoustic neuromas, conventional radiation is not effective. In this case, high-dose precision irradiation such as Gamma Knife or CyberKnife irradiation (radiosurgery), is required. The goal of this high-precision radiation is to stop the growth of the tumor. Often, the tumour can even be reduced in size a little with this method. However, as with conventional radiation, the surrounding neuronal structures (affecting the nerve cells) must be outside the irradiation field, which is ensured by planning to the nearest millimeter.
Nevertheless, effective radiation of the tumour margins is difficult. Especially in large tumours and in direct vicinity of the brain stem, such irradiation is not possible. In cases of recurrence, repeated radiation therapy is usually possible only to a limited extent. Surgical therapy is extremely difficult in tumors that have already been irradiated because of scarring of the tissue. Prof. Feigl performs radiosurgical treatment of his patients at the Cyberknife Center Southwest in Göppingen. For more information, please visit https://www.radiochirurgicum.de/cyberknife-expertenteam.php.

Understanding Acoustic Neuroma
Understanding Acoustic Neuroma
Surgical Planning with VR and 3D Technology
Surgical Planning with VR and 3D Technology

Resection of Acoustic Neuroma
Resection of Acoustic Neuroma
Request for Treatment
Request for Treatment