Understanding Pituitary Tumor
Understanding Pituitary Tumor
The pituitary, also known as the pituitary gland, is only about the size of a cherry stone, but is responsible for the main control of the entire human hormone balance. The pituitary gland produces messenger substances that regulate the hormone balance in the human body. Any disruption of this regulation can have a massive impact on those affected. Therefore, in the case of pituitary tumors, a distinction must be made between hormone-producing and hormone-inactive tumors.
The pituitary, also known as the pituitary gland, is only about the size of a cherry stone, but is responsible for the main control of the entire human hormone balance. The pituitary gland produces messenger substances that regulate the hormone balance in the human body. Any disruption of this regulation can have a massive impact on those affected. Therefore, in the case of pituitary tumors, a distinction must be made between hormone-producing and hormone-inactive tumors.
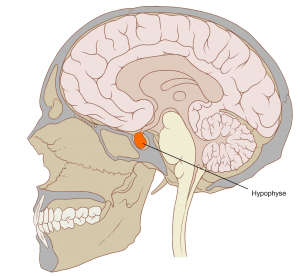
Image source: Patrick J. Lynch, original Image:Skull and Brain sagittal.svg
The symptoms of hormone-active pituitary tumors depend on the messenger substances produced by the respective tumor. Even tumors that do not secrete messenger substances, i.e. are hormone inactive, can lead to clear symptoms.
The pituitary gland is located in the center of the skull and is surrounded by many sensitive nerves and vessels. For this reason, tumors that repress these structures cause symptoms. Especially when compressing (= repressing) the optic nerves or the visual pathway crossing, large tumors cause visual disturbances and can even lead to blindness if they are not treated well and in time.
If a pituitary tumor is suspected, a neuroopthalmological examination (neuroopthalmology = focus of ophthalmology (=eye care)) of the visual acuity (vision) as well as the visual field must be carried out in addition to a detailed endocrinological examination (endocrinologist = hormone specialist). Neuroradiological imaging in the MRI (“tube”) involves thin-slice MRI images (with a layer thickness of 1 mm or less) with contrast media, native and T2 as well as CISS and specially required pituitary sequences.
The medical treatment of pituitary tumors is always performed on an interdisciplinary basis in collaboration with specialists in endocrinology and neuroopthalmology. So-called prolactinomas (= pituitary tumors that release the hormone prolactin) can be treated primarily with medication.
However, if surgery is indicated, as in the case of pituitary adenoma, Prof. Feigl removes the tumor endoscopically and minimally invasively through only one nostril using the four-hand technique, in accordance with the latest standards. Thus, no visible scars remain on the face after the operation. Prof. Feigl is an expert in this field and performs this type of surgery regularly. Neuronavigation (“GPS for the brain”) is always used in such operations at the base of the skull. Intraoperative neuromonitoring (= monitoring of brain and cerebral nerve functions) is only used in the case of very large tumors in this area and in the case of compression (= displacement) of the adjacent nerve and vascular structures.
The symptoms of hormone-active pituitary tumors depend on the messenger substances produced by the respective tumor. Even tumors that do not secrete messenger substances, i.e. are hormone inactive, can lead to clear symptoms.
The pituitary gland is located in the center of the skull and is surrounded by many sensitive nerves and vessels. For this reason, tumors that repress these structures cause symptoms. Especially when compressing (= repressing) the optic nerves or the visual pathway crossing, large tumors cause visual disturbances and can even lead to blindness if they are not treated well and in time.
If a pituitary tumor is suspected, a neuroopthalmological examination (neuroopthalmology = focus of ophthalmology (=eye care)) of the visual acuity (vision) as well as the visual field must be carried out in addition to a detailed endocrinological examination (endocrinologist = hormone specialist). Neuroradiological imaging in the MRI (“tube”) involves thin-slice MRI images (with a layer thickness of 1 mm or less) with contrast media, native and T2 as well as CISS and specially required pituitary sequences.
The medical treatment of pituitary tumors is always performed on an interdisciplinary basis in collaboration with specialists in endocrinology and neuroopthalmology. So-called prolactinomas (= pituitary tumors that release the hormone prolactin) can be treated primarily with medication.
However, if surgery is indicated, as in the case of pituitary adenoma, Prof. Feigl removes the tumor endoscopically and minimally invasively through only one nostril using the four-hand technique, in accordance with the latest standards. Thus, no visible scars remain on the face after the operation. Prof. Feigl is an expert in this field and performs this type of surgery regularly. Neuronavigation (“GPS for the brain”) is always used in such operations at the base of the skull. Intraoperative neuromonitoring (= monitoring of brain and cerebral nerve functions) is only used in the case of very large tumors in this area and in the case of compression (= displacement) of the adjacent nerve and vascular structures.
Pituitary Tumor on MRI Imaging
Examples of large Pituitary Adenomas
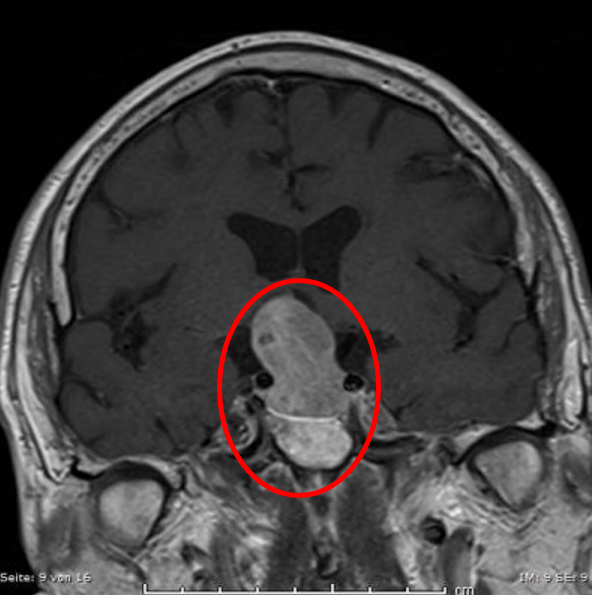
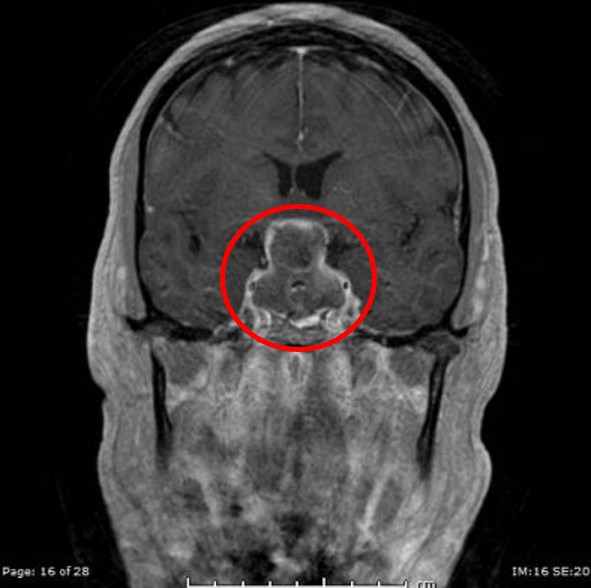

The visual pathway junction is significantly elevated (area where the optic nerves of the eyes meet).
If left untreated, this can lead to visual impairment and even complete blindness.
The visual pathway junction is significantly elevated (area where the optic nerves of the eyes meet).
If left untreated, this can lead to visual impairment and even complete blindness.

Planning of the surgery with the Surgical Theater System.
Planning of the surgery with the Surgical Theater System.
Resection of Pituitary Tumor
Request for Treatment
Request for Treatment